
By: Dr. Esteban Morales van Kwartel
PART III : J’accuse…!
When the truth is hidden underground, it becomes concentrated, acquires such explosive force that, the day it explodes, everything jumps with it.
Emilio Zolá
Note: this is a translation from an article written on 10/15/2020

INTRODUCTION
It is important to establish here that we understand, appreciate and promote the development of scientific creativity to seek appropriate measures to control the transmission of diseases, especially epidemic ones. However, we believe that efforts should be aimed primarily at avoiding or reducing mortality. In this sense, measures such as social distancing; hygiene; and detection and isolation of cases have always demonstrated, in the history of public health, since the time of Galen and before, their effectiveness in controlling diseases. The total closure of activities is, by logic and by evidence, an unjustified measure, the effectiveness of which, as is derived from what is presented in part I I of this work, has not been demonstrated with sufficient scientific evidence. On the contrary, this measure is linked to the generation of major economic upheavals, which directly generate disturbances to the well-being of people, which, directly and indirectly, generate serious public health problems.
THE COST OF QUARANTINE
According to a prestigious Swedish economic organization [1] , the global economy, in the countries of the European Community, as a consequence of the total closure (quarantine), fell by 27%, measured in terms of the “production gap [2 ]. This was considerably higher than the fall of the European financial crisis in 2010 (≈4%). It should be noted that this impact affected the sectors differently; for example, two of the sectors that represent a high percentage of jobs: hotels and restaurants; and wholesale and retail trade were among the most affected (75%), along with art, entertainment and recreation (84%). But the most alarming, according to the report, are the economic consequences that go beyond the immediate impact: permanent structural damage to the economic model and extension of the wave of economic shock to all sectors of the economy. In the United States, it was calculated that the closure of the economy would produce an output gap of 8%; it was calculated that the S&P 500 index [3] would fall to -33.9% which would represent the worst drop since the financial crisis of 2008-2009 [4] . In the month of April, in the same country, during full quarantine, the unemployment rate increased to 14.7%, after having been at 3.5%, before this measure [5]. Many times we have heard and seen writings where it is said that the economy and health are two different things that do not have to do with each other; In the specific case of this pandemic, it has been constantly repeated that everything necessary must be done to preserve health, even if the economy has to be sacrificed; even, those who have dared to say that the intervention consisting of the total closure of activities has to be suspended because it is going to produce serious consequences for humanity (which in fact are being seen), have been demonized as characters who only think about money. Those who think this way, it is because they do not know the relationship between economy, well-being and health. This has been extensively explained in our book: “Beyond Galen: Preventive and Social Medicine” [6]. Considering it of great importance in this crucial moment of humanity, we are going to make a brief summary of this.
One of the most important indicators, used by experts to measure well-being, is the so-called human development index. Among the variables that compose it there is one from the health sector, which is life expectancy at birth, and another one from the economic sector: gross domestic product (GDP). From the Declaration of Alma Ata, the concept of well-being evolves, and, later, the National Institute of Well-being of the United States, establishes 6 dimensions of this, among which is employment (economic) and the physical dimension (healthy body and health care). Researchers from the University of Davis, in the United States, establish that, having an optimal level of well-being, the individual manages to live a quality life that removes him from stress, reduces the risk of disease and ensures positive interactions.
Figure 1. Conception of health and well-being
In this new conception, HEALTH and WELL-BEING are closely related, rather amalgamated, in a mathematical relationship with two vector directions. This is easily understood insofar as we conceive of the human being as a social entity, in constant relationship with its environment, be it social, material or spiritual. Health is definitely socially determined, and to deny this is to condemn the human being unfailingly to be considered a mere social robot; in this way, we can establish the relationship between HEALTH and WELLNESS like an orange, where the peel is HEALTH and its content is WELLNESS.
Source: Morales, E. Beyond Galeno: Social and Preventive Medicine
In accordance with this, then, the deterioration of the economy, in this pandemic, has meant a deterioration of well-being, as shown in the aforementioned economic figures, which has affected health.
DIRECT EFFECTS ON HEALTH PRODUCED BY TOTAL CLOSURE
However, confinement per se, in addition to the individual and family economic deterioration that this represented and that, as experts have shown, affects well-being and, therefore, health, also had a direct effect on people’s health. In a study presented by the Atlanta Center for Disease Control (CDC), it was reported that, according to data presented by the National Syndromic Surveillance Program, which included 73% of all visits to emergency rooms in the Nation, these decreased by 42%, in the period from May 15 to May 23, 2020, compared to the period from January 5, to March 14, 2020 [7]. More importantly, the study revealed that, in the first months of the pandemic, visits to the emergency room, for all age groups and sex, for myocardial infarctions, strokes and hyperglycemic crises, decreased substantially (23%, 20% and 10%, respectively). As physicians, we know that these conditions are life threatening and require urgent attention in order to decrease their morbidity and mortality, and that the earlier they are treated, the better their prognosis. In fact, in the same article cited from the CDC, the authors refer to reports that reveal an excess of deaths, during the pandemic, not associated with COVID-19, which could be related to the situation described. They also refer to previous studies that report significant reductions in hospital admissions, by the three reported conditions, which further increases the fear of a worsening of conditions that already, in themselves, are among the major causes of morbidity and mortality in the United States and much of the world. Finally, in the study, the authors attributed this decrease in the visit of these patients to the UC emergency room to several factors, among which was the total closure, as one of them. But in addition to creating the conditions for people with risk morbidities to stop attending to their ailments, the worsening of their health status made them even more susceptible to the disease and its complications. In a study conducted in China and presented in April 2020, it was found that outbreaks of the disease, within homes, accounted for 79. 9% of all upsurges studied. They concluded that all outbreaks of 3 or more cases occurred in closed environments, confirming that sharing in closed environments is a greater risk of infection.[8]. What was done with the total confinement (quarantine) was the equivalent of placing people doused with gasoline inside an enclosure and lighting a match for them. Something similar happened with people within nursing homes, which we will refer to later.
In August 2020, the CDC published the results of a survey applied throughout the United States, conducted from June to April 2020, in the middle of the total quarantine period, revealing that symptoms of anxiety and depression disorders increased considerably in adults aged 18 years and over, compared to the same period in 2019. Overall, 40.9% of those surveyed reported having had at least one symptom. It was also reported that certain specific sectors of this population were being more affected by mental illnesses, suicidal ideas and the increase in the use of substances; among these groups, there were, in a preponderant way, adults between 18-44 years old. For example, in this group, the ideas considering suicide were significantly high (41.5%)[9] . The people nobly obeyed the orders given on the recommendation of the scientists and accepted quarantine (81.8% obedience), despite the great disruptions created to their social and work life; they were even willing to follow directions for as long as public health officials recommended (90.8%) [10]. But they failed them, abandoned them, betrayed their trust in them. Despite the fact that public health officials were aware of the dire consequences of confinement on mental health, people were left to their own devices. There was not even a serious effort to support and monitor people at mental risk, especially those prone to suicide and substance use; but worse still, it persisted in quarantine and still persists in many places. But people, especially young people, started dating; many accused them of being irresponsible and even murderers; but they were saving their life. They began to leave the room full of fuel, fleeing the flames that were approaching; but how many did not make it out? God bless them.
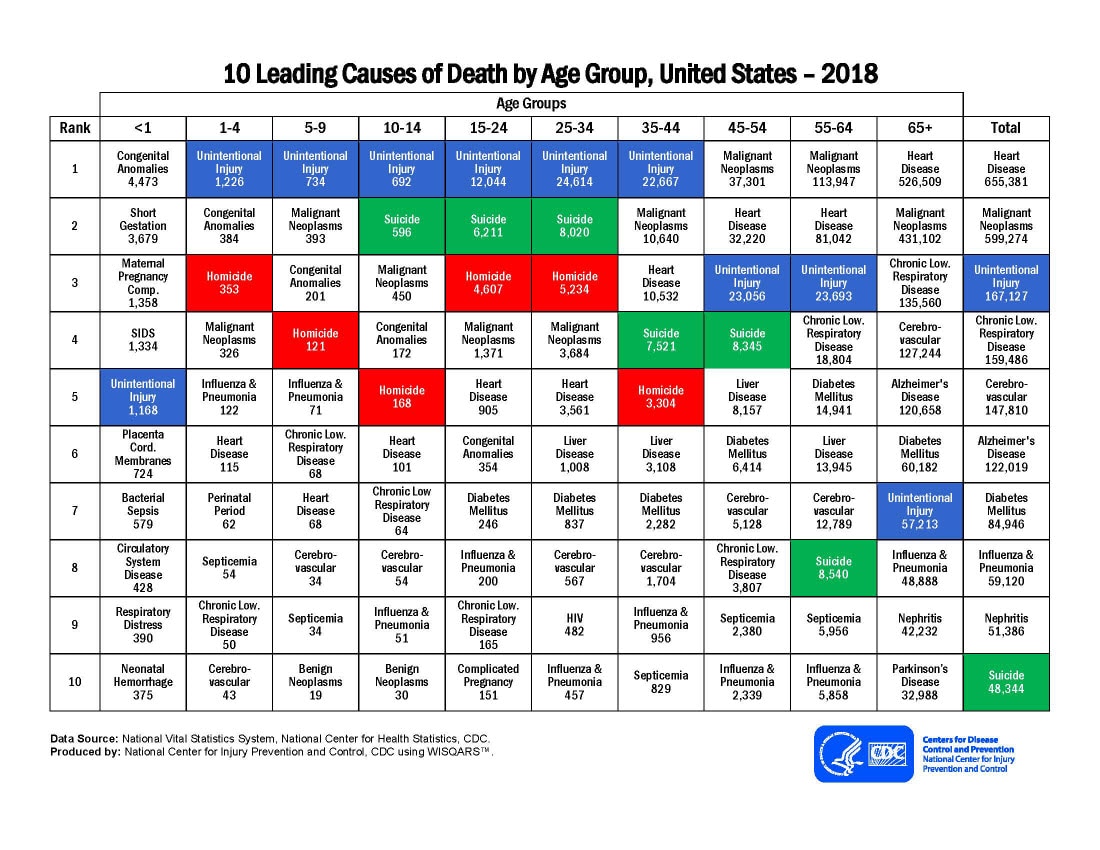
In April 2020, a study was presented in which, based on previous scientific evidence, pandemics, in general, and especially new ones, such as COVID-19, were associated with violence against women and children [11]. In that study, nine variables were identified, all of which are worsened by quarantine and isolation measures. For example, we can mention economic insecurity and problems related to poverty; inability of the woman to temporarily escape from her abusive partner; mental instability related to the disaster or pandemic situation, etc. In the case of children, as we have seen above, they have not only been exposed to the risks related to increased substance use, anxiety and depression from their parents and guardians which, as we have seen, expose them to violence , which can end in deaths, as suggested by the statistics that indicate that the first cause of death in children aged 1-18 years is unintentional injuries, but also exposes them more to cases of suicide, which , by itself, is reported as the second cause of deaths in children between 14-18 years[12] . But even worse, with the absurd and disastrous closure of schools, an action that goes against all existing scientific evidence, has put them at additional risk, by removing them from a protective environment, provided by counselors, tutors and teachers, which have been the most commonly identified and reported cases of suspected child abuse and other problems inherent to children.
In 2009, an article was published in the American Journal of Public Health describing the vulnerability of children to pandemics, in general, and in particular, the H1N1 pandemic that the world was suffering [13]. At that time, according to the article, there were 74 million children in the United States, of whom about 55 million were enrolled in schools and about 11 million in daycare. Here, reference is made to a series of studies that describe the vulnerability of children thanks to the dependence they have on adults for the attention of their needs, and their great fragility due to their growth and development that makes them subject to rigorous programs prevention of diseases, such as the application of vaccines, availability of medicines, health care and the prevention and care of mental health situations. Many of these needs are met through school programs, as well as food supplement programs through schools, of which a large number of children in poverty levels, depend for their nutrition. Despite the fact that the highest rates of infection and mortality from influenza, which was the problem at that time, occur in very young children, the study recommended avoiding, as much as possible, the closure of schools for all negative connotations that this meant for the children, and that were described in the study. However, in the face of the COVID-19 pandemic, despite numerous scientific evidence showing that infection rates in schools, among students, teachers, and administrative staff are extremely low[14], and that severe disease in children is rare, and mortality in these is very rare [15] , [16], the closure of schools was one of the first measures taken and many are still closed.
WHAT WAS NOT DONE. THE CASE OF THE ELDERLY HOMES.
Until now, the emphasis has been on counting infected people as a measure of severity, in an infection whose case-fatality rate has increasingly been revealed as extremely low over time [17]. In addition, it has been discussed and analyzed what was done and has continued to be done to control the pandemic; But it is important to talk a little about what was not done and what should be taken into account for the next epidemics that will continue to appear in the world. In a study published in the journal Nature, on the effects of non-pharmaceutical interventions in the pandemic in Europe, which we present and analyze in part II, the authors refer to the deaths occurred due to the pandemic and the deaths avoided, according to the study, thanks to a series of measures, in special, “total closure” (quarantine). But we want to emphasize what we have presented, both in the first part of this article, and in part II: the groups of people in which this mortality occurs and the reasons for this. We have spoken extensively about comorbidities and other conditions such as age (and sex), as well as risk factors for this mortality; what little is said, however, is about the main intervention that was not made (especially at the beginning of the epidemic) to face this: protecting directly, people at risk.
When we start to look deeper into the disease and noticed that lethality (which is the most important indicator of this particular pandemic), is very low, that it is basically asymptomatic and that most cases range from mild to moderate, we begin to realize the existence of the machinery of bad science in action. On May 16, 2020, an article appeared in The Guardian revealing what they described as a horrific death toll in nursing homes. According to the article, at that time, in Sweden, 50% of deaths occurred in nursing homes; in Belgium, the percentage was more than half; in Spain, deaths had been counted in only two regions and these accounted for a third of all deaths in the country, and in Italy, their figure was 40% of all deaths [18]. According to figures released by Canada’s chief of public health, deaths in nursing homes from COVID-19 accounted for 81% of total deaths from this disease in the country, prompting the Prime Minister of Canada to express: Canada is failing its elders [19]. But let’s take a closer look at two cases in particular; Sweden, for having been beaten so much for not doing quarantine (although we have already seen that, despite its high fatality figures, its decrease in Rt was within the average of the 11 countries studied), and the United States, a country immersed in a fierce political campaign where the most bizarre events that can be imagined have been taking place, and which have affected the sciences.
The case of Sweden
Sweden has been viciously attacked by many outlets, notably CNN, of course, for its high death toll from the coronavirus, basically attributing it to the denial of the application, in its country, of quarantine or total closure, and comparing this lethality with that obtained in the other Nordic countries [20]. However, in this particular interpretation of science, the already mentioned and analyzed decrease in its Rt has no longer been taken into account; besides, there was not any reference to the characteristics of deaths in the rest of the countries of the world, which we have already mentioned, and which we will continue to deepen now; and also there has not been any interest in delving into certain internal characteristics, such as those inherent to its particular structure of care for the elderly, which we will refer to later. Indeed, according to the National Board of Health and Welfare, Sweden’s official body, in charge of monitoring the development of the disease, by May 14, 2020, 90.5% of those who died from the coronavirus were 70 years or older. Of these, 86.7% had 1 or more of the morbidities that we have described in this work; only 13.3%, had no comorbidity; Of those who died from the disease aged 70 or over, more than half were 85 or over, and the percentage with comorbidities was higher. The same report cited, revealed that 79.6% of the deceased older than 70 years were in the system of care for the elderly and 88% of those older than 85 years who died, were in the system[21] . This places us in the three variables that we have been trying to highlight in this work: comorbidities, age, and elderly care services.
To fully understand what happened in Sweden, it is necessary to know how the system of care for the elderly works. This somewhat complex system is widely described in a study presented at the behest of the National Institute of Health (NIH) [22]. The system has several modalities that go, from services and facilities to be cared for in their own homes, to services of permanent residences (nursing homes); in the middle are apartment complexes dedicated to housing the elderly who do not need constant care. The most fragile elderly is housed in permanent residences, these being the ones most at risk. The report refers to previous studies where it has been revealed that the value of the median number of years remaining, from the moment of entry to permanent residences for the elderly (nursing homes), is 9 months; considering that the deceased had already been in residence for a long time, one might think that this median would have a range between 5-9 months; The most important thing about this data is that the number of deaths in this group did not vary much compared to previous years without the coronavirus. In addition to the risk factor inherent to their frailty, the factor related to the care personnel was also mentioned; This is the lowest paid service in the country and is performed in a large percentage by immigrants who, according to the study, are also people at higher risk of infection by SARS-CoV-2. Another risk factor mentioned is the so-called nosocomial, starting from the service providers, and inherent to the conditions of proximity in which the residents find themselves. Finally, it was emphasized in the study that it is necessary to learn from this experience to avoid its repetition, and that it is also important to take into account the great challenge that was given to control this, given the conditions described.
The case of the United States
In April 2020, the director of the Centers for Medicare and Medicaid Services of the United States (CMS), expressed her great concern about mortality from the COVID-19 pandemic, in nursing homes (Figure 2). At the same time, new regulations were announced, requiring greater transparency on the part of nursing homes, at all levels, including the requirement to report cases of the disease directly to the CDC, and to cooperate fully with this entity, with its surveillance efforts [23] .
Figure 2. Words from Seema Verma, CMS administrator on the effects of the pandemic in nursing homes.
Nursing homes have been ground zero for COVID-19. Today’s action supports CMS’s long-standing commitment to providing transparent and timely information to residents and their families […] Nursing home reporting to CDC is a critical component of the national COVID-19 surveillance system on-going forward and efforts to reopen America.
Source: Seema Verma, CMS News , April, 2020.
Indeed, despite early efforts made by the administration[24] , [25], on April 16, 2020, the Wall Street Journal presents an independent article where it is reported that deaths from coronavirus, in the homes of elderly, represented, at that time, at least 40% of all deaths in the country, due to the disease[26]. However, doubts are beginning to arise in the sense that this percentage could be higher, which motivated the CMS to intervene in this matter. The case of New York, in its contribution, not only to the underestimation in the registration of cases, but also in its contribution to the increase of these, was especially bizarre. According to an article published by the Associated Press[27], it is very likely that the number of deaths from coronavirus, in New York, in nursing homes, could have been strongly underestimated. One of the main reasons for this, according to the article, is that New York only counted residents who died inside nursing homes and not those who were transported to hospitals and died there. The article continues, saying that federal regulators have required nursing homes to submit data on coronavirus deaths each week, whether residents die in the facility or in a hospital, but this came after the mortality crisis. In New York; Additionally, according to federal data, approximately one fifth of the nursing homes in the State reported resident deaths from early June to mid-July, which indicates that this deficit could add thousands more dead residents in nursing homes. In addition, since the Kaiser Family Foundation, analyzing the data of 43 States (which was the number of States that sent data), found that the number of deaths from coronavirus, in nursing homes, accounted for 44% of all deaths for the disease in the country, applying this proportion to New York, this would mean that there were more than 11,000 deaths from the disease in nursing homes in that State, the article continued. The most tragic thing about this is that knowing the epidemiological reality that these institutions suffer, and that we have described above, and despite the desperate calls for help by the administrators of these institutions, the State authorities refused to support them. According to an article from the New York Post, the state governor refused to transfer infected patients from nursing homes whose numbers exceeded the capacity for assistance by its staff, to the hospital built inside the Javits Convention Center or to the hospital ship of the US Navy, the USS Comfort; these were medical facilities provided by federal support. Despite the complaints of alleged congestion at State hospitals, these facilities were always significantly under-utilized[28].
In addition to those described above, the controversy is further exacerbated by the great discomfort produced by a memo sent by Governor Cuomo, in which measures were taken that further worsen the already critical situation that nursing homes were going through. [29] (figure 3)
Figure 3. Excerpt from the memorandum sent by Governor Cuomo to nursing home administrators on March 25, 2020
No resident will be denied readmission or admission to [a nursing home] based solely on a confirmed or suspected diagnosis of COVID-19. [Nursing homes] are prohibited from requiring a hospitalized resident who is determined to be medically stable to undergo a COVID-19 test prior to admission or readmission.
Source: New York Department of Health. Memo March 25, 2020
All these situations described have prompted an investigation by the United States Department of Justice, not only in New York, but in the rest of the States; for this the United States Department of Justice, on August 26, 2020, sent an order requesting data from the governors of the States who issued COVID-19 orders that may have resulted in the death of nursing home residents[30]. Specifically, as for the State of New York, the Governor was asked to provide information on deaths of residents that could be related to the memo to which we have referred, and for which a hearing was held in August; but Governor Cuomo has refused to provide the requested information; rather, he has chosen, as is often the case with some leaders, to blame the high mortality on all the rest of humanity, except themselves: the home care personnel and the CDC for changing the norms, and not only that, but has accused the Department of Justice of political persecution[31] .
What happened, especially in New York, indicates that the mere consideration of the conditions inherent to nursing homes and the fragility of their residents were not the only factors for the rapid and high mortality of their residents. To illustrate this, we will refer to a report published by The Guardian newspaper[32], where the deaths that occurred in the United Kingdom, in nursing homes, are compared with those that occurred, in these institutions, in Germany. According to the article, the risk of death, from COVID-19, in nursing homes in Great Britain was 13 times higher than in Germany. This was attributed to the fact that, in Germany, unlike Great Britain, laboratory tests were applied from the beginning to people leaving the hospital and returning to institutions for the elderly.
SUMMARY ON THE CHARACTERISTICS OF LETHALITY BY COVID-19
This more careful look at mortality allows us to better visualize what really happened with the pandemic. As we have been focusing and penetrating the problem with increasingly higher resolution lenses, we have gradually found ourselves with a mortality characterized by a low probability of occurrence; more prevalent in people older than 70 years; especially older than 85 years; with risk comorbidities (especially NTCD); and, linked, in a high percentage, to nursing homes, especially with certain conditions. This should have been the main focus for developing the pandemic attack and mitigation strategies; it is what the most fundamental foundations of strategic programming establish. However, the strategy was totally unfocused: a massive terror was created, and everyone was locked up, without measuring the consequences, which we have been describing throughout this article. A thesis was used as justification (using models full of uncertainties), for which we have not yet been able to find the scientific evidence of its justification: flatten the curve. The experience of Sweden, and of some other countries, disqualify the variable “total closure” as effective and that, if a greater effort had been made to protect the groups at higher risk, mortality would have been much lower. The experience of Germany (where the total closure was late), and other countries, prove that the approach of action to risk groups was the correct one.
These external and unacceptable situations, described previously in the case of New York, were added to the conditions inherent to nursing homes, conditions that, for the most part, are common to these institutions throughout the world. Chris Pope, presented, in a scientific work, an exhaustive analysis of the conditions of institutions for the elderly in the United States, and that we have allowed ourselves to summarize[33]:
- Preliminary data shows that in the United States just over 2 million people lived in some type of facilities for the elderly (39% aged 85 and over), which are at high risk of infection and complications from COVID-19, due to their age and the existence of multiple NTCDs in a high percentage.
- This population has a high probability of dying quickly, even under normal conditions. Although they are 0.4% of the United States population, they nevertheless represent 19% of general mortality.
- Apart from their high mortality due to their age and comorbidities, the possibility of death from infections is high, being this, in 2016, 380,000 people in the facilities for the elderly.
- Due to their medical conditions, these people have a need to interact frequently with hospitals and other medical providers; the reduction of this interaction, due to the mitigation strategies taken, made them more susceptible to complications from their diseases.
- These institutions had a shortage of personal protective equipment, due to the priority of this for the hospitals.
- It was refused, at least in the case of New York, that, in cases of facilities congested with infected by the coronavirus, residents were transferred to other facilities.
- Unlike nursing homes in Sweden, in the United States, these facilities are not equipped with medical equipment.
- The nosocomial problem is notorious, due to the close relationship between residents and caregivers, due to the need to interact due to their physical conditions.
- Because of the existing terror due to the disease, in nursing homes there was an exodus of caregivers, producing a serious problem of care for residents.
- In New York, the population of residents in nursing homes is 1% of the population, but they accounted for 22% of COVID-19 hospitalizations (demonstrating, in our view, the fallacy of quarantining the general population for flatten the curve).
FINAL CONSIDERATIONS
What is expressed in this work highlights 4 points that we wanted to distinguish: the fragility of the majority of the victims of the pandemic; the paralyzing and disastrous panic, created irresponsibly; the weakening of community medicine, being replaced by an emphasis on hospital care; and bad science (politicization of science). As we can see, from the data presented for Sweden and the United States, most of the people who died in nursing homes were going to die within the year, probably several months later, but within the same year. We have also seen that these deaths have represented between 40 to 80% of deaths from the coronavirus worldwide. But let it be clear: it does not relieve the responsibility that greater and better measures should have been taken to protect our adult population, since human beings are not the ones who must determine who dies or not, and when. But what is very clear is that the manipulation of science, politics, and hidden interests have generated a panic in the world, which is unjustified, which resulted in extreme measures being taken that have produced immediate damage and scars that will last for a long time. This has been a pandemic of terror; It began when, for some reason, someone began to count the cases and the deaths and published them without the proper context, without the deep analysis of what was contained within the data; all this with the complicit gaze, by action, some, and, others, by omission, of a large part of the authorities, officials and workers in public health and global preventive medicine. Some for fear of the culture of cancellation, others for lack of interest in seeing beyond what the “official” organizations of world, regional and local health announced and published; both passive attitudes, which can easily be classified as cowardly.
Many of the recommendations given regarding this pandemic have been based on computer-based models, and on spurious scientific conclusions, lacking strong evidence and lacking peer review. Aspects, such as total quarantines or closures; the use of masks, of which we have not talked about in this work, due to lack of time and space; the non-reopening of schools and the economy, despite the lack of evidence that exists to maintain these measures, have become mere political flags of one side or the other. Especially in the United States, where those who want to prevent the reelection of the president, advocate the use of masks, the closure of schools, and the closure of the economy; where the discussion, based on the evidence on these issues has been corrupted. Many scientists, in particular the spokespersons of the “official” scientific bodies, supported by the “official” media, have taken their own side. Once again, the world has been left in the hands of scientists, making scientific decisions, falling into a scientific ideologization, as described by Edgardo Lander in his excellent book[34] , which undermines democracy, and which has caused great damage to humanity. We have left control of our countries and our lives to the “napoleons of science,” some of whom have had a questionable track record, in their scientific appraisal during past critical health events. However, many clinicians, public health physicians and other health workers in the community have been neglected and ignored, who did dare to express their opinions and recommendations, forgetting that we are the ones who deal with the health problems of people, and that we see life from a more comprehensive, practical and real perspective.
The latter was a sign of something even more damaging in this pandemic: not knowing that the fight against it should be carried out in the community, which was the true battlefield. In every war, the hospital is the place where the wounded and the dead are received, but the battle is fought in the community, with this pandemic, and with any other. This is based on the fact that prevention, case detection and contact traceability are carried out in the community; at the local level, where government and health workers know their population, its characteristics, its problems, weaknesses and strengths. Where, in the form of a team, the best ways to identify and protect the most vulnerable are executed. But for this, you need to have the system, and the necessary financial and personnel structure. In most of the countries this structure is significantly weakened. In the United States, with the implementation of the health reform (Affordable Care Act [ACA])[35], popularly known as Obama care, the access to health services was facilitated for the neediest people, but the meaning of the Alma Ata Primary Care strategy was distorted. According to the reform document, the emphasis is on improving access for all people to hospital care services; which is commendable; but with regard to community care services, this focused on providing services to people with fewer resources. However, according to the primary care strategy, it must be applied to all segments of the community, understood as the place where people develop, in their family and social life and where they should have access fast, close and comprehensive at all levels of care, including preventive. This includes all people, without any distinction, since all have the right, and, furthermore, all of them conditions and influences the epidemiological components. Concepts of health, in the United States, such as the so-called “Medical Home”, have suffered a profound and serious lack of financial and human resources that has led to their ineffectiveness. This, which, more than a concept, is a model of Primary Care, is described in our book: Beyond Galen: Preventive and Social Medicine. We will speak more extensively in the fourth installment of this article about the strategy to attack the epidemic, specifically about things to do and other public health recommendations, as we believe that we must be better prepared to face the next epidemics that are going to arrive.
Finally, we want to emphasize that we citizens do not elect scientists to govern us; our rulers, the majority, however, have also sinned by omission, neglecting their responsibility to make the correct decisions for the well-being of the people who elected them, leaving these in the hands of scientists. This, we recognize, is not easy, but for that they were chosen; thepolitically correct is easier but irresponsible. However, this is not the first time it has happened; It has been occurring with other fundamental issues in our world, such as climate change. Here, too, statistical models have been used strongly questioned by the enormous number of uncertainties, confounding variables, etc., that we have described in this work. We have also denounced it in our recently published book: The two great scientific frauds of the 20th and 21st centuries. This pandemic has the prospect of going down in history as the greatest scientific fraud of humanity. From there, our J’accuse…!
References
[1] Copenhagen Economics, ECONOMIC CONSEQUENCES OF THE COVID-19 PANDEMIC (Copenhagen, Sweden) <https://www.copenhageneconomics.com/dyn/resources/Publication/publicationPDF/0/530/1585835646/copenhagen-economics_economic-consequences- covid-19.pdf > [accessed 3 October 2020].
[2] The production gap, usually called “output gap” is the percentage difference recorded in a given time between the GDP of the economy and potential GDP, which is one that would obtained with a “normal” use of productive resources without generating macroeconomic imbalances. From: https://guiasjuridicas.wolterskluwer.es/Content/Documento.aspx?params=H4sIAAAAAAAEAMtMSbF1jTAAASMjExNTtbLUouLM_DxbIwMDS0NDA7BAZlqlS35ySGVBqm1aYk5xKgCpfpK1NQAAAA==WKE#:~:text=La%20brecha%20de%20la%20producci%C3%B3n%2C%20denominada%20normalmente % 20output% 20gap% 2C% 20es, productive% 20without% 20generate% 20ofimbalances% 20macroecon% C3% B3mic .
[3] This index is based on the stock market capitalization of 500 large companies that own stocks listed on the NYSE or NASDAQ, and captures approximately 80% of all market capitalization in the United States. It is one of the most indicative of the real market situation. Viewed at: https://es.wikipedia.org/wiki/S%26P_500
[4] The Council of Economic Advisers, Evaluating the Effects of the Economic Response to COVID-19 (Washington DC., 2020) < https://www.whitehouse.gov/wp-content/uploads/2020/08/Evaluating- the-Effects-of-the-Economic-Response-to-COVID-19.pdf > [accessed 3 October 2020].
[5] US Bureau of Labor Statistics, ‘Unemployment Rate Rises to Record High 14.7 Percent in April 2020: The Economics Daily: US Bureau of Labor Statistics’, US Bureau of Labor Statistics , 2020 < https://www.bls.gov /opub/ted/2020/unemployment-rate-rises-to-record-high-14-point-7-percent-in-april-2020.htm > [accessed 12 October 2020].
[6] Morales. Esteban, Beyond Galeno: Preventive and Social Medicine , Editions (Panama: Novo Art SA, 2016).
[7] Mmwr / June and others, Morbidity and Mortality Weekly Report Potential Indirect Effects of the COVID-19 Pandemic on Use of Emergency Departments for Acute Life-Threatening Conditions-United States, January-May 2020 , 2020, xxvi < https: / /www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics- > [accessed 5 October 2020].
[8] Hua Qian and others, ‘Running Head: Indoor Transmission of SARS-Cov-2 Indoor Transmission of SARS-CoV-2’ < https://doi.org/10.1101/2020.04.04.20053058 >.
[9] Mark É. Czeisler and others, ‘Mental Health, Substance Use, and Suicidal Ideation During the COVID-19 Pandemic – United States, June 24–30, 2020’, MMWR. Morbidity and Mortality Weekly Report , 69.32 (2020), 1049–57 < https://doi.org/10.15585/mmwr.mm6932a1 >.
[10] Mark É Czeisler and others, ‘COVID-19: Public Compliance with and Public Support for Stay-at-Home Mitigation Strategies’ < https://doi.org/10.1101/2020.04.22.20076141 >.
[11] Amber Peterman and others, Pandemics and Violence Against Women and Children , 2020 <www.cgdev.org > [accessed 6 October 2020].
[12] CDC, ‘Leading_causes_of_death_by_age_group_2018_1100w850h.Jpg 1,100 × 850 Pixels’ < https://www.cdc.gov/injury/images/lc-charts/leading_causes_of_death_by_age_group_2018_1100w850h.jpg > [accessed 6 October 2020].
{kind=link}
[13] ‘Pandemic Influenza Planning: Addressing the Needs of Children’ <https://doi.org/10.2105/AJPH.2009.159970 >.
[14] https://statsiq.co1.qualtrics.com/public-dashboard/v0/dashboard/5f62eaee4451ae001535c839#/dashboard/5f62eaee4451ae001535c839?pageId=Page_1ac6a6bc-92b6-423e-9f748a-259a
[15] CDC COVID-19 Response Team, Coronavirus Disease 2019 in Children – United States, February 12 – April 2, 2020 , 2019 < https://www.cdc.gov/coronavirus/2019-ncov/downloads/pui-form .pdf .> [accessed 6 October 2020].
[16] Zunyou Wu and Jennifer M. McGoogan, ‘Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China’, JAMA , 323.13 (2020), 1239 <https://doi.org/10.1001 /jama.2020.2648 >.
[17] https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios.html?fbclid=IwAR3DvH5umpJxiObUDTKBckeBAfqudrtvzWfQhYiUfHeEhCFeg5UXzalabGg#box1
[18] ‘Across the World, Figures Reveal Horrific Toll of Care Home Deaths | Coronavirus Outbreak | The Guardian ‘, The Guardian (London, UK, 16 May 2020) <https://www.theguardian.com/world/2020/may/16/across-the-world-figures-reveal-horrific-covid-19- toll-of-care-home-deaths > [accessed 7 October 2020].
[19] Amanda Coletta, ‘Canada’s Nursing Home Crisis: Coronavirus Killing in Long-Term Care – The Washington Post’, Washington Post (Washington DC, May 18, 2020) <https://www.washingtonpost.com/world/the_americas/ coronavirus-canada-long-term-care-nursing-homes / 2020/05/18 / 01494ad4-947f-11ea-87a3-22d324235636_story.html > [accessed 8 October 2020].
[20] Emma Reynolds, ‘Sweden Says Its Coronavirus Approach Has Worked. The Numbers Suggest a Different Story – CNN ‘, CNN.Com (Atlanta, April 18, 2020) <https://www.cnn.com/2020/04/28/europe/sweden-coronavirus-lockdown-strategy-intl/index .html > [accessed 8 October 2020].
[21] https://www.socialstyrelsen.se/globalassets/1-globalt/covid-19-statistik/engelska-sidan/statistik-covid19-avlidna-engelska.xlsx
[22] Charlotta Stern and Daniel B Klein, ‘Stockholm City’s Elderly Care and Covid19: Interview with Barbro Karlsson’ < https://doi.org/10.1007/s12115-020-00508-0 >.
[23] Centers for Medicare & Medicaid Services, ‘Trump Administration Announces New Nursing Homes COVID-19 Transparency Effort | CMS ‘, CMS News (Washington DC, April 2020) < https://www.cms.gov/newsroom/press-releases/trump-administration-announces-new-nursing-homes-covid-19-transparency-effort > [ accessed 9 October 2020].
[24] Centers for Medicare & Medicaid Services, ‘CMS Prepares Nation’s Healthcare Facilities for Coronavirus Threat | CMS ‘, CMS News (Washington DC, February 2020) <https://www.cms.gov/newsroom/press-releases/cms-prepares-nations-healthcare-facilities-coronavirus-threat > [accessed 9 October 2020].
[25] Centers for Medicare & Medicaid Services, ‘CMS Announces Actions to Address Spread of Coronavirus | CMS ‘, CMS News (Washington DC, March 2020) <https://www.cms.gov/newsroom/press-releases/cms-announces-actions-address-spread-coronavirus > [accessed 9 October 2020].
[26] Jon Camp and Anna Wild, ‘As US Nursing-Home Deaths Reach 50,000, States Ease Lockdowns – WSJ’, Wall Street Journal (New York, June 16, 2020) <https://www.wsj.com/articles/ coronavirus-deaths-in-us-nursing-long-term-care-facilities-top-50-000-11592306919 > [accessed 9 October 2020].
[27] Associated Press, ‘New York’s True Nursing Home Coronavirus Death Toll Cloaked in Secrecy’, Associated Press , 2020 < https://www.foxbusiness.com/lifestyle/coronavirus-nursing-home-death-toll-new-york > [accessed 9 October 2020].
[28] Bernadette Hogan, Karl Campanile, and Bruce Golding, ‘New York Nursing Home Denied Requests to Send COVID-19 Patients to USNS Comfort’, Washington Post (Washington DC, April 24, 2020) < https://nypost.com/ 2020/04/24 / new-york-nursing-home-denied-requests-to-send-covid-19-patients-to-usns-comfort / > [accessed 9 October 2020].
[29] Andrew Cuomo and Governor, ‘Department of Health of New York-MEMO. March, 25, 2020 ‘(Albany, NY, 2020). https://dmna.ny.gov/covid19/docs/all/DOH_COVID19%20_NHAdmissionsReadmissions_%20032520.pdf
[30] Department of Justice Office of Public Affairs, ‘Department of Justice Requesting Data From Governors of States That Issued COVID-19 Orders That May Have Resulted in Deaths of Elderly Nursing Home Residents | OPA | Department of Justice ‘, Press Release Number: 20-828 , 2020 < https://www.justice.gov/opa/pr/department-justice-requesting-data-governors-states-issued-covid-19-orders-may -have-resulted > [accessed 9 October 2020].
[31] Morgan MCKay, ‘Justice Department Investigating Nursing Home Deaths in NY’, Spectrum News (Albany, 26 August 2020) < https://www.ny1.com/nyc/all-boroughs/politics/2020/08/26 / us – justice-department-investigating-nursing-home-resident-deaths-in-ny > [accessed 8 October 2020].
[32] Robert Booth, ‘Covid-19: Risk of Death in UK Care Homes 13 Times Higher than in Germany | World News | The Guardian ‘, The Guardian (London, UK, 28 June 2020) <https://www.theguardian.com/world/2020/jun/28/covid-19-risk-of-death-in-uk-care- homes-13-times-higher-than-in-germany> [accessed 8 October 2020].
[33] Chris Pope, ‘Nursing Homes Are Ground Zero For Coronavirus’, City Journal (New York, May 2020) <https://www.city-journal.org/coronavirus-super-spreaders-nursing-homes> [accessed 8 October 2020].
[34] Edgardo Lander, Science and Technology as Political Issues Limits of Democracy in the Technological Society , Editorial (Caracas, Venezuela: Faculty of Economic and Social Sciences of the Central University of Venezuela (FACES), 1992) < https: //www.tni.org/files/download/ Science and technology as political issues.pdf > [accessed 9 October 2020].
[35] Office of the Legislative Counsel, COMPILATION OF PATIENT PROTECTION AND AFFORDABLE CARE ACT] INCLUDING PATIENT PROTECTION AND AFFORDABLE CARE ACT HEALTH-RELATED PORTIONS OF THE HEALTH CARE AND EDUCATION RECONCILIATION ACT OF 2010 PREPARED BY THE (Washington DC., 2010) < http://docs.house.gov/ > [accessed 13 October 2020].